
Much of the misinformation and confusion surrounding Covid-19 relates to whether the vaccines are safe and effective.
It is completely understandable to have questions, and no-one should be dismissed for wanting to find the best information out there. I will do my best, using all the available evidence, to cover some of the questions I’ve seen, along with the myths and misinformation that are floating around.
There are some fantastic resources explaining how the vaccines work, which I won’t cover. The AstraZeneca vaccine is explained with great diagrams here, and the Pfizer one here.
“If vaccines are so ‘safe’ then why are the vaccine companies not responsible for paying for compensation, like they are for medicines?”
In the 1970s a little girl developed polio after taking the live polio vaccine. This was a known but very rare possibility (far less likely than her chances of developing polio without the vaccine). However, the doctor had not warned her father about it, so the father sued the company and won his case.
This set a precedent for people to sue vaccine makers if they believed they had been affected adversely by the vaccine. Unfortunately, it is impossible to prove a negative, so as long as the symptom developed shortly after the vaccine was given, the vaccine was assumed to be the cause.
Unsurprisingly, this led pharmaceutical companies to become reluctant to develop vaccines, as the huge legal costs of compensating anyone who claimed a vaccine injury, added to the immense costs of developing the vaccine to begin with, made it financially unviable. So governments stepped in and set up vaccine-injury compensation programmes to deal with the payments, allowing the drug companies to get back to developing much-needed vaccines.
This has led to an inflated public awareness of ‘vaccine injury’, far more than any fears or discussion surrounding medicinal side effects. Despite all the claims in the US, in around 70 per cent of the compensation cases the committee agreed a settlement “in which they had not concluded, based upon review of the evidence, that the alleged vaccine caused the alleged injury.”
For some perspective: in the US (a very litigious society) around 300 million doses of vaccines are administered every year, with around 300 successful claims made to their compensation programme. Only around 30 per cent have shown any evidence of a link, suggesting around one in 4.5 million vaccinations result in injury. This is a vanishingly tiny risk, compared to the risk of contracting the diseases the vaccines are preventing.
“The vaccine trials have been too quick – no one knows what the long-term side effects will be.”
There are two types of potential ‘long-term side effects’: a reaction to the vaccine that has long-term lasting effects, or an effect that won’t been seen for a long time after the vaccination occurs. The former would be picked up by phase three clinical trials, the big studies where thousands of volunteers receive either the vaccine or an inactive placebo. These trials allow the effects of the vaccine to be compared to those who didn’t receive the vaccine, as well as being able to check for any side effects, which would develop shortly after the vaccine was given. Side effects not seen when thousands of people have received the vaccine will be very rare.
The Pfizer/BioNTech trials included 43,000 volunteers and the AstraZeneca trials included 20,000 volunteers, and in both cases the only side effects seen were common vaccine reactions such as headache, sore arm, and tiredness.
Between those trials, and since starting to vaccinate the public, millions of people have now received the vaccine and so far, there have been no major adverse events. So if there is the possibility that one of these vaccines will cause a long-term side effect, it will be a one in a multiple million chance of happening. This should certainly not be a reason to risk catching Covid-19, which has up to a one-in-10 chance of long-term health problems.
As for the second type of side effect – one where you don’t develop symptoms until years after the vaccine – that has only ever been seen with one vaccine: the chickenpox vaccine. The nature of that vaccine means that in rare cases the live attenuated virus (modified virus that can trigger the immune system but is unable to cause disease) can lie dormant and, years later, lead to cases of shingles. It should be noted that getting chickenpox itself is far more likely to lead to the development of shingles in later years.
None of the Covid-19 vaccinations being developed involve this type of vaccine, so there simply isn’t the possibility that this will happen.
So to sum up, if there were to be any long-term side effects of the Covid-19 vaccines, we would have seen them during the trials, or else they are so rare that they should not affect your decision to vaccinate.
“The vaccines have been developed too quickly – they must have cut corners.”
The vaccines have been through the same rigorous clinical trials as any other vaccine and have been proven to be safe. Tens of thousands of volunteers (and now hundreds of thousands of people a day) have had the vaccines and there has been no evidence of any major safety issues. Issues with vaccine safety are generally seen within days or a few weeks of having the vaccine and, so far, none have been reported.
Some people are concerned by how fast these vaccines have been developed, rightly questioning: how come it has happened in less than 12 months when it usually takes years? The answer is vast sums of money, scientific collaborations, more people researching them than ever before, the high prevalence of the virus in the community, and the unprecedented decision to make the vaccines before the trials were complete, so they would be ready to go.
Vaccine trials usually take years because each step happens after the next one: research, followed by getting authorisation to run a trial, followed by recruiting patients, followed by waiting for enough people to be exposed to a disease to see if the vaccine is working, followed by analysis, followed by reporting, followed by more authorisations, followed by finally being allowed to make and use the vaccine. In this case, the number of volunteers, the amount of virus circulating, the money and desire to find a vaccine haven’t been in short supply, which have made all these steps happen faster, but no less rigorously.
“The Covid-19 vaccines are killing people.”
In early January 2021, reports came out of Norway that 33 people in care homes had died within a week of receiving the Pfizer vaccine. This understandably caused a scare in the press. However, the Norwegian Institute of Public Health and the WHO (World Health Organisation) have both confirmed that there was no link between the vaccines and the deaths. 55,000 elderly people in Norway had received the vaccines at that point. 45 people in that age group die every day in Norway, meaning 33 deaths out of 55,000 people vaccinated is not unexpected.
During clinical trials, there were two deaths in the Pfizer vaccine group (compared to six in the placebo group), both of which were investigated and found to be unconnected to the vaccine.
According to the American VAERS (Vaccine Adverse Event Reporting System), a site where you can register any side effects (‘Adverse Events’) you believe were caused by the vaccine (from a sore arm right through to death). Of the 21 million US citizens to receive at least one dose of either the Pfizer or Moderna vaccine by the middle of January, only 196 deaths were reported. It is important to note that each of these deaths is then investigated further, to establish whether the death is a result of the vaccine or not. So far there have been no deaths attributed to the vaccine.
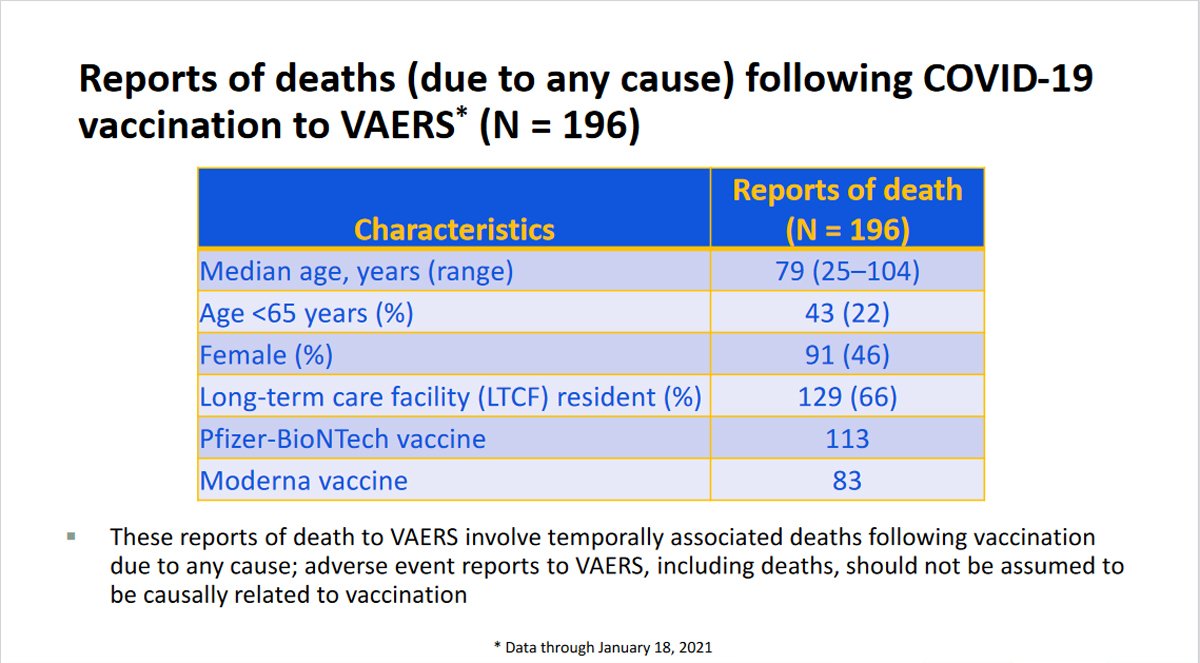
Of the 196 deaths reported, 129 took place in care homes. Based on the age profile of the residents, and the number who were vaccinated, you would statistically expect 11,440 deaths in the timeframe of the post vaccination period, so 129 deaths being reported should not be cause for alarm. It is also interesting to note that mortality in the vaccinated residents of care homes was lower than the unvaccinated residents in the same care homes, and also lower than in the care homes yet to be vaccinated.
In the UK, we see around 1000 deaths each day in the over 80s and the under 80s in care homes and over 80s in the community. Given that this is the age group we are vaccinating first, it is extremely likely that we will see deaths following the vaccination purely by chance, and so caution should be used if you hear stories of people dying after receiving the vaccine.
“The Covid-19 vaccine causes infertility”
Claims were made that the vaccine targeting the Covid-19 spike protein would also train your body to attack syncytin-1, a protein found in the placenta, because they shared a short amino acid sequence (amino acids are the building blocks of proteins). This would lead the immune system in pregnant women to attack the placenta, leading to miscarriage, and prevent any future pregnancies.
The claim is totally unfounded on multiple levels. Firstly, the shared sequence is so small it is like suggesting that the fact you have the number seven in your phone number means anyone dialling an 11-digit number with a seven in it will connect to you! If you were to compare the sequence of the spike protein to any protein in the human body you will, by chance, find some parts that match. But there is no evidence that Covid-19 antibodies are targeting every protein in your body – if that was the case then infertility would be the least of your worries!
And secondly, if antibodies to the spike protein were causing infertility, you would expect infertility to result from contracting the disease itself. Millions of people across the world have now had Covid-19 and there is no evidence at all that fertility has been affected. We also know that in the Pfizer trials, 12 vaccine volunteers got pregnant, compared to 11 in the placebo group.
Of the 21+million people who had received at least one dose of either the Pfizer or Moderna mRNA vaccines in the USA by late January, more than 15,000 had reported a pregnancy to the vaccine monitoring body, so it’s pretty clear the vaccine is not causing infertility.

“The Covid-19 vaccine will alter your DNA”
This is simply not true. In order to do that, the mRNA would need to enter the nucleus of the cell (where your DNA is stored), which it can’t do without a ‘nuclear access signal’, which it doesn’t have. Even if it did get in (which it can’t), it would then need to be turned into DNA, which needs something called ‘reverse transcriptase’, which it doesn’t have. And even if it did get in (which it can’t) and turned itself into DNA (which it can’t), it would then need something called ‘integrase’ to insert itself into your DNA, which – you guessed it – it doesn’t have!
Imagine your DNA is a recipe book for how to make every protein in your body. mRNA is like a photocopy of the recipe for the protein you want to make. Photocopies are made all the time and fed into ‘machinery’ that can read the recipe, and make the protein required.
The Pfizer and Moderna vaccines contain one of these photocopies (mRNA) from the virus, which is designed to enter your cells, (not the nucleus), and tell your protein machinery how to make one part of the virus and display it on the outside of the cell. Your body then recognises this as an intruder and makes antibodies to it. If you then get infected by the real Covid-19 virus, your body is already prepared to fight it, helping eliminate it much more quickly.
So, although the mRNA enters your cells, it not only gets nowhere near your DNA, but it is also not possible for mRNA to alter DNA, any more than a photocopy of a recipe can alter the recipe book itself.
“The Covid-19 vaccine will give me Covid-19”
None of the Covid-19 vaccines contain the virus itself and so cannot infect you with Covid-19. They all use different methods of introducing just the spike protein of the virus to your immune system. The spike protein alone cannot reform into the complete virus.
“People are suffering all sorts of horrendous side effects after having the vaccine, which the government is trying to keep hidden.”
Both parts of that statement are untrue.
There are multiple different surveillance operations set up to pick up, monitor and track any side effects. These form the most intense and comprehensive vaccine safety programme in history. In the UK, the Medicines and Healthcare products Regulatory Authority (MHRA) has a ‘Yellow Card’ scheme, where any member of the public can report suspected side effects. The COVID-19 Vaccine Safety Technical (VaST) Subgroup in the US meets weekly to review all available data and has reported on larger numbers than the UK. They monitor self-reported events, community surveillance programs, and doctor-reported events. Initially they are relying on VAERS (Vaccine Adverse Event Reporting System), the site where you can register any adverse effects following the vaccine. It is important to note that both the “Yellow Card” and the VAERS are sites where anyone can register an event, with no proof they’ve even had the vaccine, let alone evidence that the effect was caused by the vaccine. This leaves it open to abuse from people wishing to spread mistrust of the vaccines.
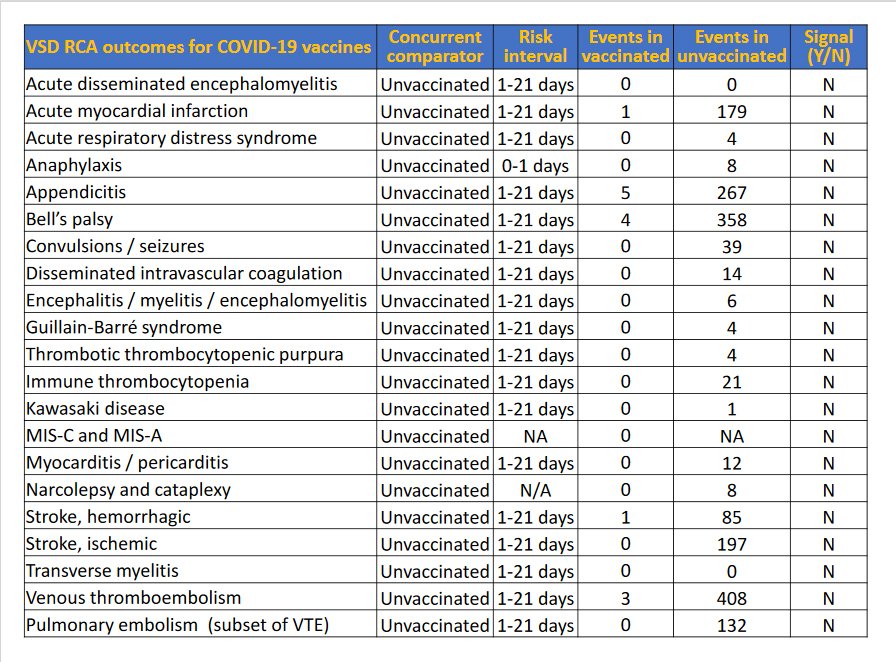
Bearing all that in mind, there had been 979 reported Serious Adverse Events (AE), and 8,117 reported non-serious Adverse Events by the middle of January in the US, following 21 million doses of the vaccine having been administered. Below are tables taken from Advisory Committee on Immunization Practices (ACIP) January 27, 2021 showing the most commonly reported non-serious AE and the Serious AE reported. The second table compares the number of reports of each event with how many times you would expect to see that event happening by pure chance in an unvaccinated population of the same size.
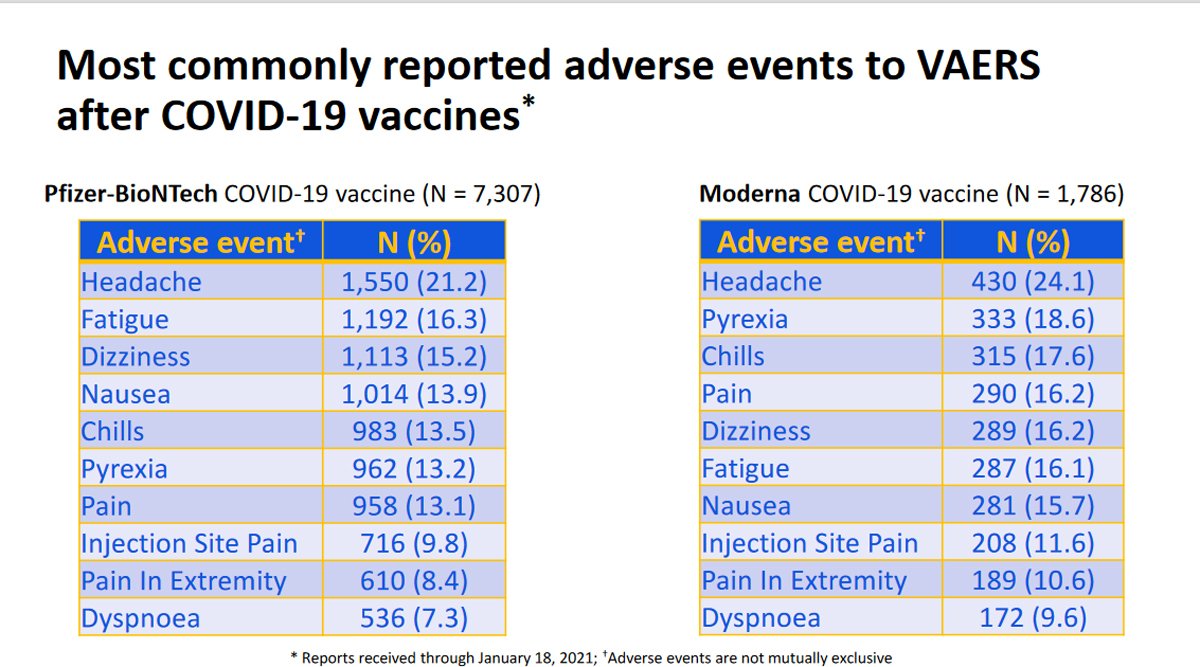
So people are experiencing some mild side effects, which are to be expected following any vaccination, including a sore arm, mild headache, dizziness etc. But there have been no serious side effects linked to the Covid-19 vaccine so far, despite millions of people having been vaccinated, with the exception of some cases of a severe allergic reaction (anaphylaxis) following vaccination. This was seen in some of the early vaccinated population, was very quickly raised as a potential issue, and is being monitored very closely. It is thought to occur in between 2.8 and 5.0 per million doses, so very rare. But in response to the issue, it has been recommended that patients should be checked for risk prior to vaccination and monitored for symptoms post-vaccination.
‘Yellow Card’ data in the UK is also being analysed, and has shown similar patterns to the data seen in the US. No deaths have been linked to the vaccine so far, and no serious side effects have been observed at any greater frequency than in a non-vaccinated population. The idea that anyone is trying to hide the side effects is simply not true. With clinical trial patients continuing to be followed up, multiple programs set up to allow both self-reporting and medical professional reporting, not to mention the world’s press waiting to jump on any story surrounding the vaccines, we can be very reassured that if there were any problems, they would be picked up fast. The anaphylaxis response shows how that works.
“The COVID-19 vaccine contains microchips”
No, they really don’t! There is absolutely no evidence that the vaccines contain microchips. Nor any evidence that injected microchips would be able to control you. This is all science-fiction-type thinking.
The idea that scientists, governments, doctors, and the regulatory bodies approving the vaccines, would all collaborate across the world to inject people with microchips, and not a single person would go public with that information, is ludicrous. All the big tech companies are already able to track pretty much everywhere we go using our phones and everything we buy or look at online, so they really don’t need injectable microchips to achieve that!
“The Covid-19 vaccine contains cells from aborted foetuses and monkey DNA”
This is a myth seemingly based on a misunderstanding about the Astra Zeneca vaccine and how it is created. The vaccine is made from an adenovirus (a type of virus that causes colds in chimpanzees) that is genetically altered. Firstly, this is to make sure it cannot cause infection, and secondly to add the genetic code for the Covid-19 spike protein. When this is injected into the body, our immune system gets primed to defend against the spike protein, giving us protection if we get infected by Covid-19.
Adenoviruses need to be grown in cells and scientists discovered some cells, called HEK293 cells, that were particularly good at growing adenoviruses, forming mini adenovirus factories. The first HEK293 cells came from a foetus aborted for personal reasons in 1973. The cells being used today grew from these original cells – but are not the exact cells from the foetus.
As the adenoviruses replicate inside the cells, they burst out, destroying the cells in the process. The adenovirus is then purified, removing all cell fragments, to create the vaccine. So although the vaccine is manufactured in these cells, there are no foetal cells in the vaccine itself. And although the idea of foetal cells sounds upsetting, it’s important to realise that no pregnancies have been terminated to produce them.
As for the ‘monkey’ DNA, again this seems to be a misunderstanding. The vaccine contains DNA from a virus known to infect chimpanzees. It does not contain chimpanzee (or monkey) DNA.

In conclusion, there is, unfortunately, a huge amount of misinformation out there; some based on misunderstandings, but sadly some being spread in a deliberate attempt to persuade people that Covid-19 is not that serious, and to put people off being vaccinated. This is extremely dangerous during a global pandemic, which is why it is so important to get your facts from reliable sources.




