
As you may already be aware, we have been reporting on the abysmal treatment of the clinically (extremely) vulnerable (CEV/CV), especially since so-called ‘Freedom Day’. Now Johnson has declared a premature end to Covid mitigations in what is clearly a political move to shore up his rapidly-vanishing support. There is no basis for such a reckless, dangerous move in the science.
The pandemic is not over. Ending restrictions does not mean it’s over. Ending reporting of the figures does not make the cases, the hospitalisations or the deaths suddenly stop. The BBC asked if it was brave or foolish to end the measures to control the spread of this rapidly changing, aggressive virus with its potential for long term organ damage. What could possibly be brave about putting lives at risk to save a mucky, shoddy political career?
We are writing to express our grave concern regarding the absence of layers of scientifically-proven mitigations which, if implemented, provide a robust defence against Covid-19 infections in schools.
Updated evidence proves the danger Covid-19 poses not just to adults but also to children. We ask that the risk to life, including orphanhood, the risk to health, including repeated infection and the resulting impairment of life chances be recognised. The government could and should utilise reasonable and proportionate measures to avoid placing schools in a position where they unknowingly in breach the Human Rights Act, the Disability Act NI , the Equality Act 2010 , the Public Sector Equality Duty , the UN Convention on the Rights of The Child and Health and Safety Law.
As many people who are Clinically Extremely Vulnerable, Clinically Vulnerable (CEV/CV) and/or immunosuppressed or immunocompromised have a protected characteristic, schools need urgent and up to date guidance on the implementation of reasonable adjustments according to EA2010.
The consequence of reopening schools with an inadequate risk assessment is evident in the government’s own statistics. According to the most recent data from the Department for Education, a staggering 400,000 children are absent from school and missing in-person education. This disruption to education is affecting the life chances of a generation of children, causing unnecessary stress.
This can be rectified by immediately implementing proven mitigations into schools.
1 in 13 primary school aged children are infected with Covid-19 and 1 in 8 children are absent from school. (Imperial REACT-1 Study, 26 January 2022)
On the 16th of September 2021, Professor Whitty stated that “Covid-19 is not a benign disease in children”. The growing body of the government’s own data supports the Chief Medical Officers statement from last year. Research, emerging continually, supports rather than refutes the need for caution.
3.98 million confirmed child Covid-19 cases since the pandemic began. It is estimated that 1in 7 have or will develop Long Covid
145 child Covid-19 deaths in the UK as of 2.2.22 , 50% of whom lost their lives since Freedom Day. NB: these numbers are subject to further research and verification.
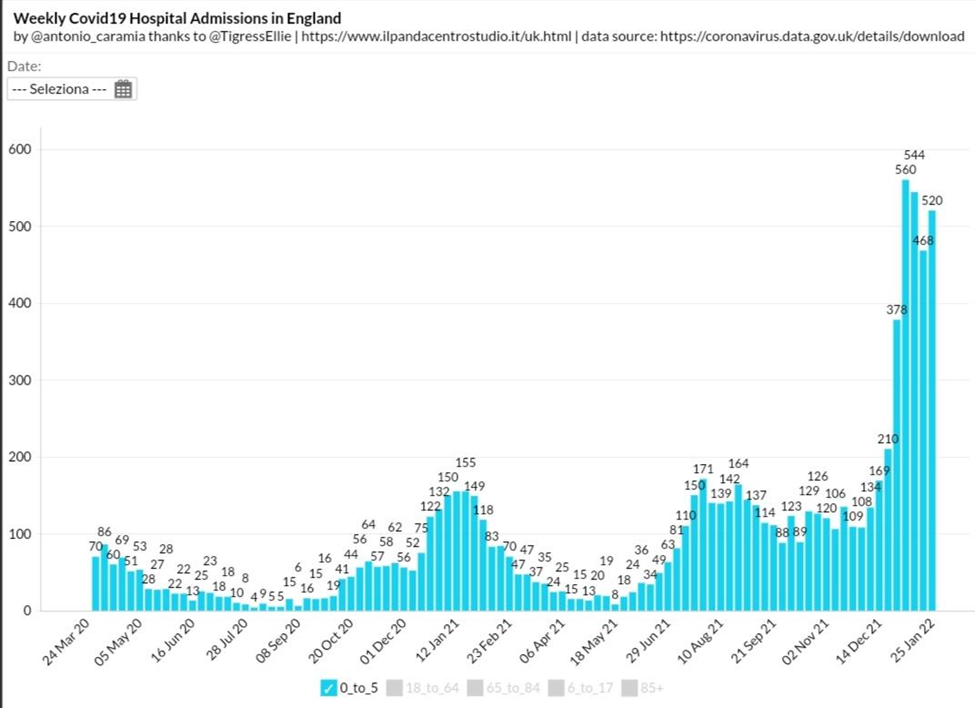
18,200 children have been hospitalised in England, of whom half were aged five or under.
New child covid cases have consistently account for around 30% of all new cases since January 2022.
Long Covid is the enduring legacy of this novel neurotropic virus.
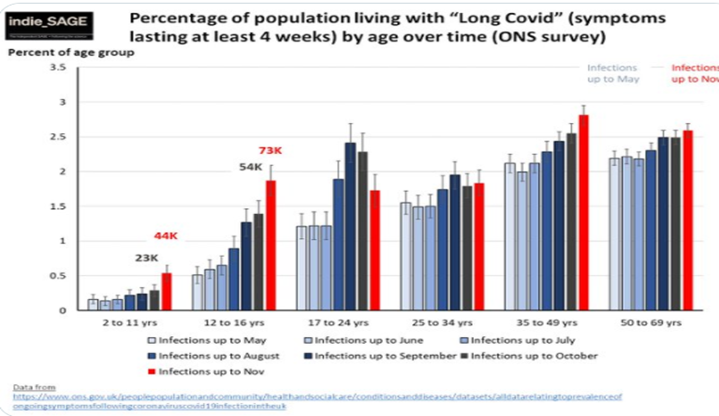
The ONS prevalence study estimates indicate that 117,000 children and young people are living with Long Covid; 20,000 of whom are still experiencing symptoms after 12 months. NIHR review on Long Covid identified these distinct syndromes
- Long Term Organ Damage
- Post Viral Syndrome
- Post ICU Syndrome
- And, potentially, an entirely novel syndrome specifically and uniquely identified as Long Covid
In addition,Covid-19 has been identified as causing the following:
- Myocarditis,
- Neurocognitive impairment,
- New type I and Type 2 diabetes cases.
This evidence raises concern of the possibility of a new cohort of Clinically Extremely Vulnerable and Clinically Vulnerable
There are an estimated 3.8 million Clinically Extremely Vulnerable and clinically vulnerable people (CEV/CV) in the UK. Early in the pandemic, people with greater clinical risk of covid19 complications and mortality were identified. Many were asked to go into shielding in March 2020 yet as the pandemic progressed and the risk for certain conditions more evidenced, the list was not fully updated and problems highlighted with the algorithm as reported by the BMJ.
Further characteristics that put people at risk of mortality and severe disease include deprivation, ethnicity, disability, obesity, being male and people over the age of 60. Shielding and status were removed in the summer of 2021. This left 91 per cent to continue self-shield or take extra precautions whilst being written out of policy and guidelines. This has resulted in pressure on family relationships as well as damaged trust with schools and employers. The public sector equality duty states that good relations should be fostered. With the end of supported shielding, many had to choose between following potentially life-saving clinical advice or their income. SSP (statutory sick pay) has been exhausted and many now face food and fuel poverty. We know of CEV/ CV families who have lost their homes and many more have a vastly reduced quality of life due to the stress caused by lack of policy across all sectors.
We are reliant on a vaccine-only approach yet we know vaccine protection wanes. We have a cohort unable to have the vaccine at all due to contraindications. There are also 800,000 immunosuppressed and immunocompromised children, young people and adults. We can see from the Octave study that many have a poor vaccine response showing few or no antibodies. Additional guidance for this cohort was issued December 24th 2021 including:
- Continue to follow any condition-specific advice you may have been given by your specialist.
- Work from home if you can.
- Avoid enclosed crowded spaces.
- Practice social distancing if that feels right for you and your friends.
- Ventilate your home by opening windows and doors to let fresh air in.
- Ask friends and family to take a rapid lateral flow antigen test before visiting you
- Ask home visitors to wear face coverings.
Covid-19 is officially designated an airborne disease, yet mask mandates have been scrapped, placing life and health at risk. We would like to highlight a section from the government’s own recent guidance:
“Schools, as employers, have a duty to comply with the Equality Act 2010 which includes making reasonable adjustments for disabled staff. They also have a duty to make reasonable adjustments for disabled pupils, to support them to access education successfully.
No pupil should be denied education on the grounds that they are, or are not, wearing a face covering.”
According to this guidance schools:
- must comply with health and safety law
- must update risk assessments
- must abide by the Equality Act 2010
Sarah Hammett QC, a Public Law and Human Rights Barrister with particular expertise in education, was asked by the Good Law Project to provide urgent advice to clarify whether the Secretary of State could ban schools from choosing to continue to use masks. Two crucial points emerged from her response:
“It is important for schools to realise that” IV 18. Guidance is not law”
and
“28 (v) “Consideration is given to the effect on disabled pupils and staff, and necessary adjustments under the equality act are in place”
Schools must promote fully-informed, parental and child choice on the wearing of masks. Despite the lack of a child-focused awareness campaign, parents, children and young people are willing to mask where the science supports this. It is crucial to note that some people may not be fully aware of their own risk and may be unaware that there is a duty towards reasonable adjustment. The Children’s Commissioner’s Back to School Guide places emphasis on washing hands and sneezing into a tissue.
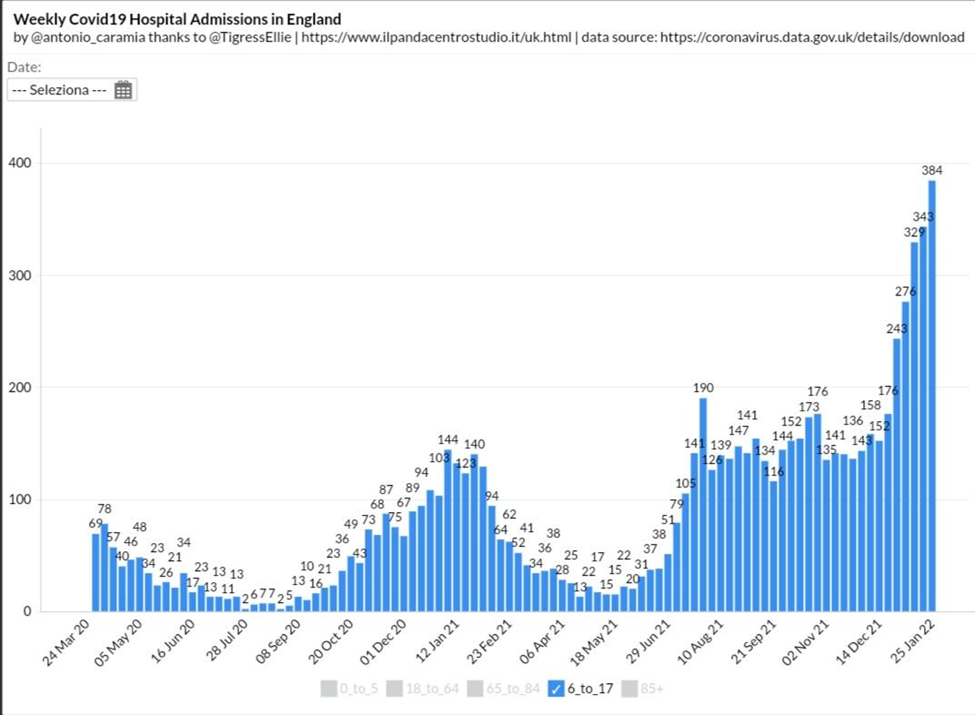
The Department of Education’s blog permits mask removal on the basis that cases are on a downward trajectory despite cases rising in school as proven in the data above. There is no guidance on the protection afforded to the individual and their family by using a good quality mask to mitigate airborne transmission, nor of the need to reduce risk for vulnerable groups.
Doughty Street Chambers has written on the Rights of The Child in the Pandemic. They have shown that the UN Committee is clear on the right to accurate information on infection prevention. The government ratified the UNCRC in 1991 and by doing so recognises the child’s rights to expressing and receiving information.
We would like the information improved to include up to date symptom presentation, aerosol transmission and the efficacy of N95/ FFP3 masks, as well as inclusion and awareness of risk for clinically vulnerable and immunosuppressed pupils, families and staff, and an updated risk for all children given the rate of hospitalisation, long covid and death.
The Children’s Commissioner has a special duty to vulnerable children including young carers. The Department of Education, the Children’s Commissioner, schools and LEAs all have an obligation under the Equality Act 2010 and the Public Sector Equality Duty. Many people who are at higher risk from coronavirus are vulnerable due to a protected characteristic be it disability, ethnicity or age.
We are aware that school is the only safe place for some vulnerable children and we fully support the role school plays in safeguarding them. However, we are concerned that this should not be at the expense of mitigations nor breach the Equality Act and Health and Safety Law. If we want attendance to be paramount, we must make schools Covid-safe for ALL children.
Many CEV/CV families were left with no remote learning when granted the ability to shield. There has been no equity in education throughout the pandemic. Although the guidelines to schools acknowledge that there are children who will still be unable to attend under clinical advice due to vulnerability to covid, we believe this to be too narrow a statement as not all children are under consultant care. It also removes the power of child and parental choice while community transmission is high and fails to consider CEV/CV parents. It is imperative that all have equal access to education and that full educational provision is available.
Committees with responsibility for interpreting the UN human rights covenants and conventions have called for the continuation of the right to education, “including distance learning, to continue access to education, particularly for children and adolescents. Students with disabilities should also have equal access to the same education opportunities.”
UNICEF has warned that children with disabilities “may be at risk of exclusion from education if remote / distance learning programmes are not accessible or they do not have assistive devices to allow participation and accommodate learning needs”. UNICEF gives examples of assistive devices such as: talking calculators, text magnifiers, alternative keyboards and audio books.
We know of families still awaiting laptops from the first wave. A lesson to be learned from the pandemic is that children can remote learn. One of our missions is to have an AV1 robot in every Local Authority for the children who cannot attend school. Pre-pandemic, it’s estimated that a quarter of a million UK children miss at least 14 school days each year due to long term illness. We must build on the positive advances we have made.
We agree that in person education has many mental health benefits and that schools are integral for many SEND children to access essential therapy. We are aware that isolation through school closures can have a detrimental impact. We also ask that the mental health impact of bereavement be fully considered, mitigated against and transparently discussed in policy and guidance from the outset. According to a Lancet study 8886 children in England and Wales were orphaned to coronavirus by February 2021 alone; two children were double orphaned. We would like the mental health impact of hospitalisation and ICU included, as well as the wider trauma of losing a classmate, a teacher or becoming debilitated by Long Covid.
The term ‘Covid anxiety’ is becoming widely used and does not reflect the fact that for our CEV CV families we are still at risk, our young carers carry the fear of bringing Covid home to a vulnerable family member, that our 5+ are struggling to access the vaccines and our immunosuppressed do not have the protection they need. This is not ‘Covid anxiety’ and we feel this is a discriminatory term; we have been told our risk, we know our own health, we are asked to mitigate our own risk, but do not have the power to do so especially in our schools. In the last quarter of 2021, 9,135 people died due to Covid, and of that number 7,559 or 84.2 % had pre-existing conditions. We are often dismissed as the minority but in terms of fatalities, we are the majority.
Recommendations:
There is still time to intervene and reduce further stress, pain and loss.by implementing the following recommendations:
- Mask-wearing: to be permitted and encouraged for all. Education on the efficacy of good quality masks and the benefits to the wearer to be provided. Children and school staff who are CEV/CV or live with someone who is, to be allowed to wear masks in line with reasonable adjustments under the Equality Act 2010 to be seen in the context of eliminating discrimination, advancing opportunity and fostering good relations under the Public Sector Equality Duty. We would also include reasonable adjustments under EA2010 to be implemented in situations with high aerosol transmission, such as exemption from assemblies and indoor P.E.
- Installation of HEPA filtration units in ALL rooms in all schools in recognition of Covid-19’s now official classification as an airborne disease. Ensure all mechanical ventilation is sufficient for room size and occupancy. C02 levels to be monitored in every schoolroom that does not yet have a HEPA filter and a plan of action should levels exceed 800 ppm.
- Vaccination: The option of full vaccination for all children, guidance issued urgently to parents/caregivers/clinicians on how to book the vaccine, accurate information for clinicians and ensuring time is given to acquire protection
- Support: CEV/CV families and all other child cases granted access to remote learning. all fines, prosecutions and threats ceased in line with their right to Education, Private Family Life and Duties under the Equality Act. CEV/CV families are entitled to invoke these rights as proven by The Good Law Project’s challenge and agreed by Nadhim Zahawi, “confirming that the provision which allows schools to authorise absences in exceptional circumstances – “regulation 7” – does apply to Covid-related absences, including children who are vulnerable or live with vulnerable family members.”
- Information: Daily LFTs in schools and weekly PCR tests. We have seen many with positive PCR tests but continuing negative LFTs. LFT are an important measure but cannot and must not be fully relied upon for the safe opening of schools. Schools to be sent a weekly breakdown of UK-wide case numbers, hospital admissions, Long Covid cases and fatalities in children. School leaders must have up to date accurate information in order to effectively protect the health and lives of students and staff.
Human Rights are universal and inalienable, indivisible, interdependent and interrelated. Article 2 of the Human Rights Act safeguards everyone’s right to life and ensures that we do not balance the worth of one life against another. Article 14 ensures they are applied without discrimination.
If our schools and public buildings are made safe for our most vulnerable, then they are safe for everyone. Investment in our children’s future health and education must be the first priority and our Human Rights must underpin all decisions moving forward.





