
After weeks of speculation on whether or not children aged 12-15 would be offered a Covid-19 vaccination, the Joint Committee on Vaccinations and Immunisation (JCVI) finally released their report on 3 September. As is often the case, the findings widely reported in the press didn’t fully reflect what the report actually said, and this has led to a lot of confusion, particularly in parents who want to know if they should get their children vaccinated (as and when that becomes an option). I will do my best to pull together, objectively, all the relevant science to help with that decision-making process.
Have the vaccines been approved for use in 12-15 year olds in the UK?
Yes. On the 4 June 2021, the Medicines and Healthcare Products Regulatory Authority (MHRA – the body that ensures that medicines are safe, effective and of good quality in the UK) approved the use of the Pfizer vaccine for 12-15-year-olds. Following Pfizer’s clinical trial in that age group, they concluded that: “the Pfizer/BioNTech Covid-19 vaccine is safe and effective in this age group and that the benefits of this vaccine outweigh any risk. It will now be for the Joint Committee on Vaccination and Immunisation to advise on whether this age-group will be vaccinated as part of the deployment programme.” The Moderna vaccine was also approved for 12-17 year olds on August 17, 2021.
So basically, they concluded it was safe and effective, but the decision on whether or not it was worth rolling out a mass vaccination programme in this age group would be up to the JCVI.
What did the JCVI report conclude?
They concluded: “The benefits from vaccination are marginally greater than the potential known harms. The margin of benefit, based primarily on a health perspective, is considered too small to support advice on a universal programme of vaccination of otherwise healthy 12 to 15-year-old children at this time.”
Digging a bit deeper into the report, there were some issues that I think are important to discuss regarding what they did and didn’t consider when coming to this conclusion.
What numbers did they base their calculation on?
As soon as their report came out, a number of scientists quickly pointed out what they believed to be significant flaws in the calculations used to determine the risks from Covid to adolescents. One member of Independent SAGE, Deepti Gurdasani, tweeted “The JCVI analysis of benefit vs risk of vaccines in children doesn’t even pass the most basic scrutiny. Bizarrely, despite their massive errors in analysis, *hugely* underestimating risks to children even they find that benefits outweigh risks but decide not to vaccinate them!”
Dr Gurdasani queried why they only looked at hospital and Intensive Care Unit (ICU) admissions and not deaths (there have been 11 deaths from Covid in this age group, compared with zero from vaccines). Even more worrying, the risks of ICU admission used in their calculations appeared to be out by a factor of five (their number suggested we would have seen around 17 ICU admissions for Covid-19 so far, when in reality, there have been 91).
The JCVI disagree that their methods are flawed and say they will publish details in due course. In the meantime, it looks as if they have ignored the risk of death and underestimated the risk of severe disease in this population. Despite this, they still concluded the benefits of the vaccination outweighed their calculated risks.
What side effects did they look at?
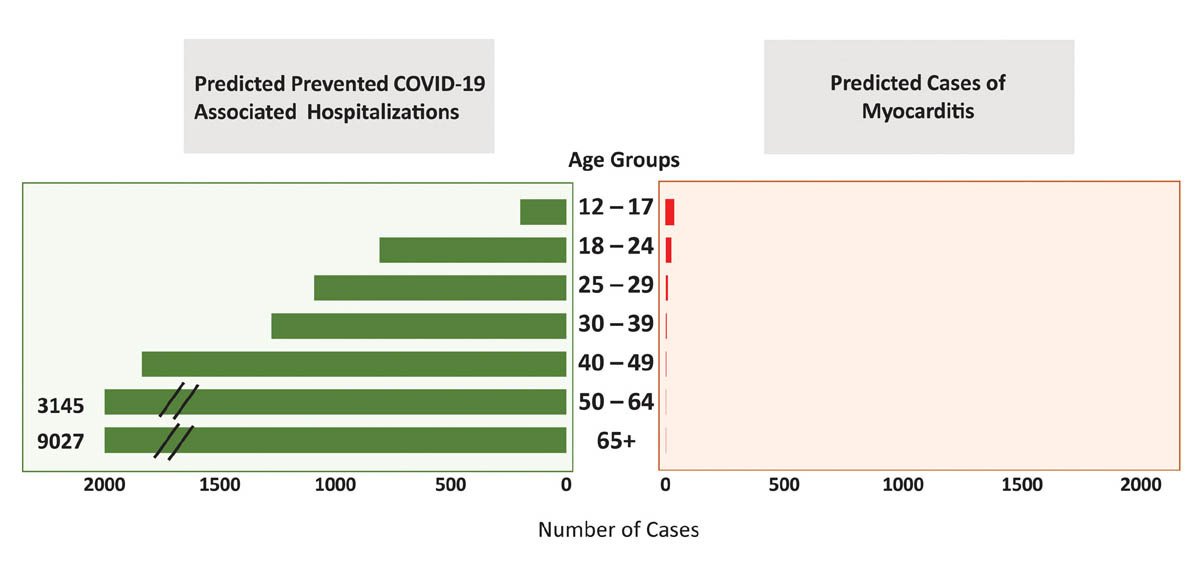
The data from over nine million children who have been vaccinated in this age group in the US, Canada, Australia and much of Europe show that, so far, the only serious side effect is myocarditis, which seems to be particularly elevated in adolescent boys following their second dose of the Pfizer or Moderna vaccine.
In almost all cases, this inflammation of the heart muscle has been shown to diminish again with or without treatment. A detailed report into this risk concluded that: “Despite rare cases of myocarditis, the benefit-risk assessment for COVID-19 vaccination shows a favourable balance for all age and sex groups; therefore, COVID-19 vaccination is recommended for everyone ≥12 years of age.”
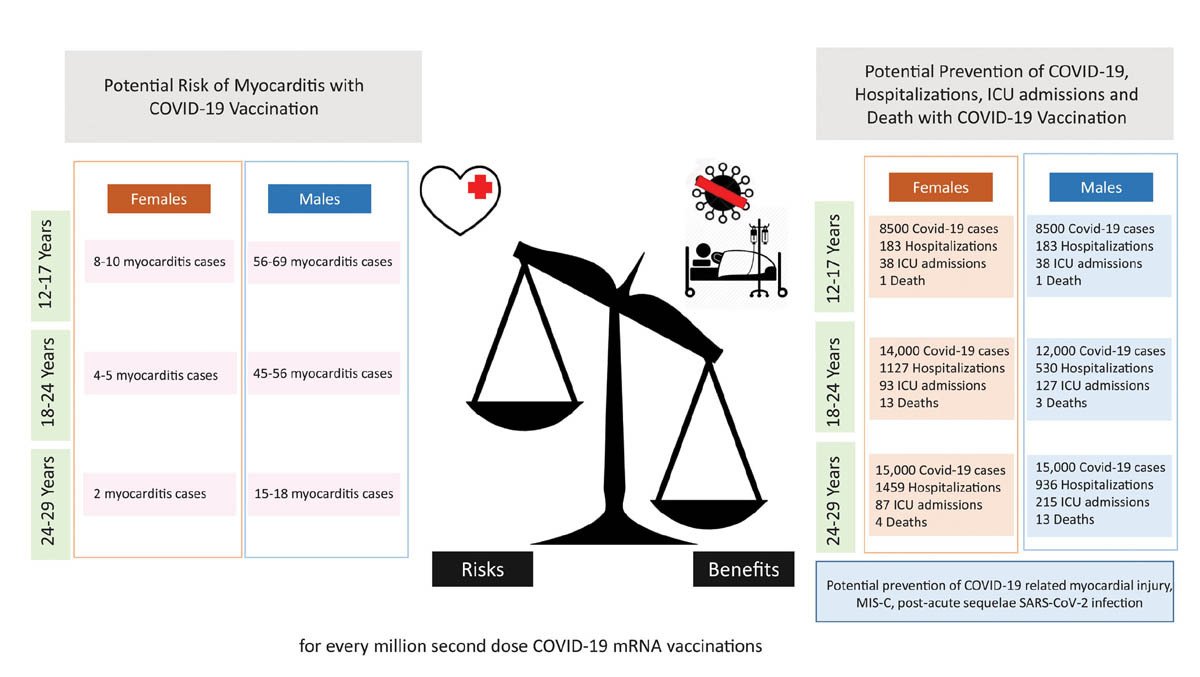
It is also important to note that while the mRNA vaccinations have been shown to increase the risk of myocarditis, being infected with Covid-19 gives a six times higher risk of myocarditis. This type of increase in risk following infection compared to vaccination was found to be true of a range of potential side effects.
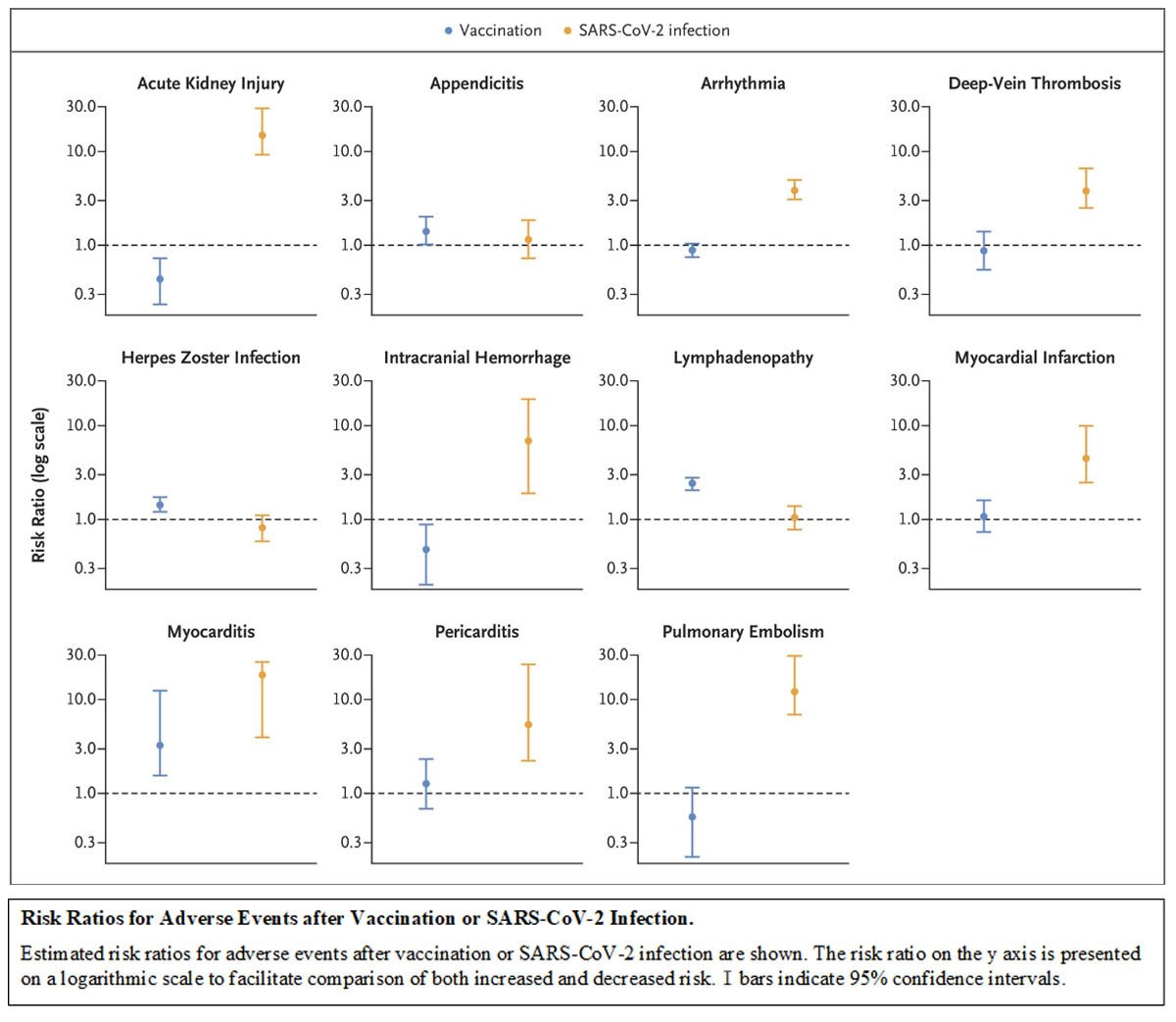
https://www.nejm.org/doi/full/10.1056/NEJMoa2110475
What about long-term side effects?
The lack of long-term data on the safety of the vaccinations in children was given as an area of caution by the JCVI. Many people worry about the vaccines having some sort of side effect in the future, which we don’t yet know about.
However, with only one exception I am aware of, vaccines simply don’t work like that. Medication can lead to unknown side effects years later as the levels in your body increase over time. But with vaccinations, the components are injected, they activate the immune response, and are then cleared from your body within days or weeks. There is, quite literally, nothing left to trigger a ‘side effect’ years down the line. (The only exception to this is a vaccine based on a weakened live virus which does remain in your body and can, in rare circumstances, revert back to a more aggressive version. However, none of the Covid-19 vaccines involve any virus, live or dead!).
For all other vaccines, side effects occur within days or weeks of the vaccination. We have a really good understanding of what the possible side effects are, based on data from 12 million children (aged 12-17) and three billion people worldwide who have received a vaccine so far. Anything we have yet to see would be so vanishingly rare as to be almost negligible. We know about myocarditis, blood clotting issues and some allergic reactions. We’ve used this information to decide which groups should have which vaccine and what to look out for following the jab.
Impact of a vaccination programme
Strangely, the JCVI mentioned that a vaccination programme would impact the education of children as they would need a short amount of time out of class to receive the vaccination (as is routine for other teenage vaccination programmes) and may need some time off due to mild side effects such as headache and fever. However, they made no reference to the disruption of education from actually catching Covid-19 and having to then isolate for 10 days!
Impact of Long Covid
One glaring omission from their report was any mention of Long Covid. Two recent studies looked at rates of Long Covid in children and young people specifically.
The study from Kings College London, based on parents reporting their children’s symptoms using the Zoe Covid-19 app, found around 1 in 20 children still had symptoms after 28 days and 1 in 50 still had symptoms after eight weeks.
The study from UCL and PHE, based on questionnaires sent to children who tested positive for Covid-19 (and those who tested negative to form a control group), found that as many as one in seven children still had symptoms after 15 weeks, significantly more than in the control group. Both groups had very similar mental health scores, suggesting the symptoms were not anxiety-driven as has been suggested by some in the media.
The numbers obviously differ between the studies, as they used different methods of data collection, but whether you use the one in seven, or the one in 20 value, there are potentially several children in every class in every school in the country suffering weeks of headaches, fatigue and brain fog following infection.
The latest ONS data suggests 2.5 per cent of all secondary aged children currently have Covid-19 (data from before the schools returned). With nearly four million children currently in secondary school, that’s roughly 100,000 currently infected children of that age group, which could lead to a potential 14,000 cases of Long Covid JUST from children infected this week!
These high numbers are the reason why 15 specialist Paediatric Long Covid units are being set up across the UK. It’s a very real and worrying consequence in children who contract Covid-19. For it not to have been even considered in the JCVI calculations is simply baffling.
Would the vaccine really make a difference to the rates in children?
Pfizer undertook a clinical trial with 2000 volunteers aged 12-15, and saw no Covid-19 cases in the vaccinated group and 16 cases in the placebo group, which shows very real benefits.
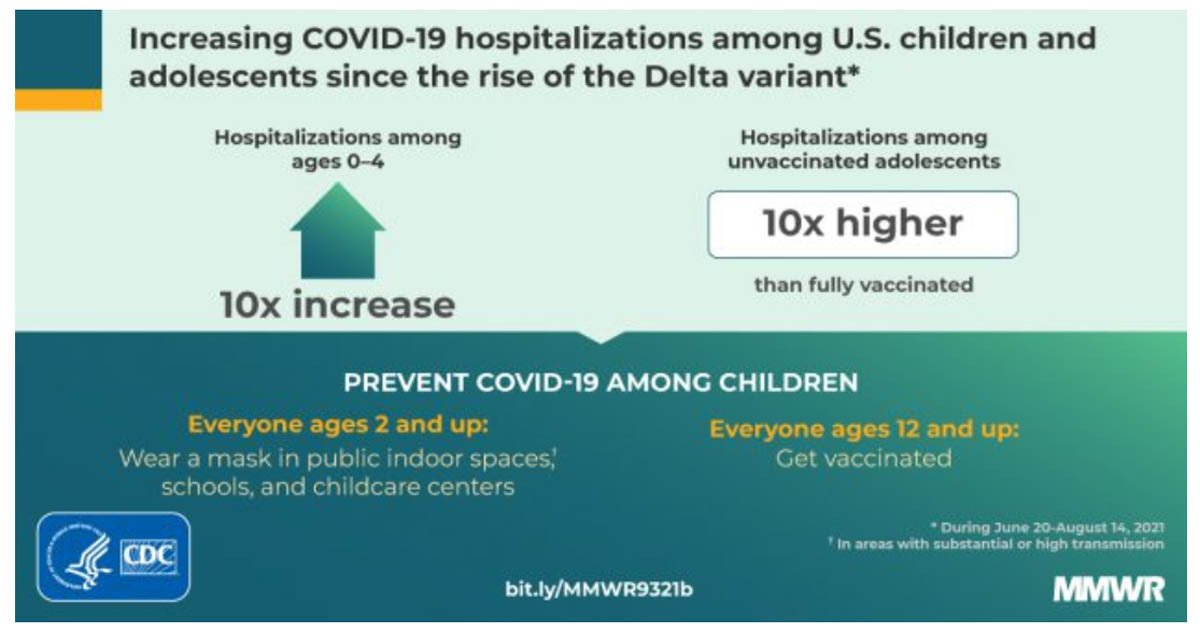
The latest real world data is from the Centre for Disease Control in the US, where they have been vaccinating 12-15-year-olds for several months now, since arrival of the more highly contagious Delta variant. It shows that hospitalisation rates are 10 times higher in unvaccinated teens than the vaccinated.
So, yes, I’d certainly argue the data shows there is a definite benefit to vaccinating teenagers.
Transmission
The JCVI stated that their report was only going to look at the direct benefits and risk of vaccination on the child being vaccinated. They said, very specifically, that they were not looking at the benefits to the wider population, such as peers, teachers and older family members.
Bizarrely, they claimed: “Understanding of the current and future role of schools on wider transmission, due to the previous use of non-pharmaceutical interventions, increases this uncertainty about the potential impact of vaccination.” In short, they are saying they cannot be certain what the effects on transmission in schools will be, as we have not had children in school with no masks, no bubbles, no contact isolations… I would hazard a guess that transmission rates won’t be less than when those mitigations were in place!
The original vaccine trial results, back in 2020, didn’t look at the vaccines’ ability to reduce transmission, or even whether they stopped you from catching it in the first place. As a consequence, there appears to be a widely held belief that the vaccines “don’t stop you getting Covid-19 and you can still spread it”. And many parents therefore feel that there is little point in vaccinating their children, who are at very low risk from Covid-19 itself, if they can still infect others.
However, since January this year, there have been numerous studies from all over the world showing that the vaccinations really do impact transmission. A study from Oxford in April 2021 showed a 65 per cent reduction in ALL infections (not just symptomatic ones) and a reduction in transmission to others in the community following the start of the vaccination programme. A recent study from University of Illinois showed vaccinated individuals who did get infected were LESS likely to shed infectious virus and they shed for a SHORTER period of time compared to unvaccinated individuals. Another study by Public Health England, found that people were 40-50 per cent less likely to contract Covid-19 from an infected, vaccinated, household member than an unvaccinated one. There have been many more studies, all showing that if you are vaccinated, you are less likely to pass on a Covid-19 infection if you do become infected, which in itself is less likely to happen than if you weren’t vaccinated.
So, although the JCVI only looked at the direct benefit to the child being vaccinated, it is impossible to ignore the wider benefits to the community as a whole – those children who cannot be vaccinated for medical reasons, those in their families who may be vulnerable, those adults in schools who may be more susceptible. The vaccines don’t offer complete protection against Covid-19, but the more people are vaccinated, the lower everyone’s risks become. This is the basic concept behind herd immunity. Without vaccinating children, many scientists believe we can never reach herd immunity for Covid-19.
Conclusion
There is a lot of puzzlement in the scientific world regarding the JCVI findings. The MHRA approved the vaccine 12-15 months ago and there is three months-worth of teenage vaccination data from the US, Canada and much of Europe, and nine months-worth of adult vaccination data. However, the JCVI want to wait another three months so they can take a ‘cautionary’ approach.
There are unlikely to be any new side effects that we haven’t already seen having given out 5.5 BILLION doses worldwide so far! Over a quarter of a million 6-17-year-olds have contracted Covid-19 and more than 1000 of them have been hospitalised in the UK with the virus since the MHRA approved the vaccine for teenagers back in June. Imagine how many more will be affected while we wait for more data.
The ‘cautionary’ approach is the right approach in normal times, but when you have a safe, effective vaccine approved for use in teenagers, and you can protect them from infection, long covid, hospitalisation or even deaths, now is not the time to ‘wait for more data’, especially when there is almost no chance that new data will emerge, given that 12 million teenagers have already been vaccinated safely worldwide.
Dr Gurdasani explains here how the cautionary approach has let us down in the UK time and again during the pandemic; delaying implementation of masks, accepting airborne transmission, asymptomatic transmission etc, and how this is yet another example where waiting for ‘perfect’ data is actually doing more harm than good.
We know the vaccine is safe.
We know side effects are generally mild, with the rare myocarditis being both temporary and also more likely to occur following infection than the vaccine.
We know the vaccine protected volunteers in the trials as well as offering really good protection using real world data.
We know the JCVI have used risk calculations that appear to underestimate the risks of infection to children, ignoring the actual number of deaths and hospitalisations, long covid, the educational disruption from contracting Covid and having to isolate: yet still they found the benefits of vaccination outweighed the harms to the child.
And we know there will be further reaching benefits to society from vaccinating teenagers, not examined in the report.
The JCVI report concluded by saying: “The government may wish to seek further views on the wider societal and educational impacts”. It is really important to understand that their report was only designed as advice, and they readily accept that the government may go ahead with vaccinating teenagers once they have taken advice from other fields.
The danger is that this may get framed as the government ‘going against scientific advice’ which could lead to a lot of vaccine hesitancy among parents and children.
The ‘scientific consensus’ from around the world (including our own MHRA) is that the vaccine is safe and effective, and the benefits far outweigh the risks. In this instance, the JCVI is very much the outlier in not recommending it.




